The muscles of the leg are organized into three fascial compartments.
The anterior compartment primarily contains muscles that produce extension (dorsiflexion) and inversion; the posterior compartment primarily contains muscles that produce flexion (plantarflexion) and inversion; and the lateral compartment primarily contains muscles that produce flexion (plantarflexion) and eversion.
A. Cross-section of the right leg. B. Movements of the ankle. C. Muscles of the anterior compartment of the leg.
Actions of the Ankle
The ankle (talocrural) joint consists of articulations between the tibia and talus (tibiotalar joint) and the fibula and talus (talofibular joint) and allows for motion primarily in the saittal plane, as (Figure 37-1B) follows:
- Plantar flexion (flexion). Movement in which the angle between the leg and foot increases.
- Dorsiflexion (extension). Movement in which the angle between the leg and foot decreases.
The subtalar joint is formed by articulations between the talus and the calcaneus and allows for motion primarily in the coronal plane, as follows:
- Inversion (prontation). Movement in which the plantar surface of the foot faces medially.
- Eversion (supination). Movement in which the plantar surface of the foot faces laterally.
Muscles of the Anterior Compartment of the Leg
The muscles of the anterior compartment of the leg produce numerous actions because some muscles cross the ankle, foot, and digits, and perhaps a combination of each of these joints (Table 37-1). The muscles in the anterior compartment of the leg have the following similar features:
- Common innervation. Deep fibular nerve.
- Common action. Dorsiflexion.
- Common vascular supply. Anterior tibial artery.
Muscle |
Proximal Attachment |
Distal Attachment |
Action |
Innervation |
|---|---|---|---|---|
Anterior compartment of the leg |
||||
Tibialis anterior |
Tibia and interosseous membrane |
Medial cuneiform and base of metatarsal 1 |
Dorsiflexion of foot at ankle joint; inversion of foot |
Deep fibular n. (L4, L5) |
Extensor digitorum longus |
Fibula and lateral tibial condyle |
Via dorsal digital expansions into digits 2–5 |
Extension of lateral digits 2–5 and dorsiflexion of foot |
Deep fibular n. (L5, S1) |
Extensor hallucis longus |
Fibula and interosseous membrane |
Distal phalanx of great toe |
Extension of great tow and dorsiflexion of foot |
|
Fibularis (peroneus) tertius |
Distal part of fibula |
Base of metatarsal 5 |
Dorsiflexion and eversion of foot |
|
Lateral compartment of the leg |
||||
Fibularis (peroneus) longus |
Upper surface of fibula |
Medial cuneiform and base of metatarsal 1 |
Eversion and plantarflexion of foot |
Superficial fibular n. (L5, S1, S2) |
Fibularis (peroneus) brevis |
Lower surface of fibula |
Base of metatarsal 5 |
||
Posterior compartment of the leg (superficial group) |
||||
Gastrocnemius |
Medial head: superior to medial femoral condyle Lateral head: superior to lateral femoral condyle |
Via calcaneal tendon to posterior surface of calcaneus bone |
Plantarflexes foot and flexes knee |
Tibial n. (S1, S2) |
Plantaris |
Superior to lateral femoral condyle |
|||
Soleus |
Posterior aspect of tibia (soleal line) and posterior aspect of fibular head and shaft |
Plantarflexes the foot |
||
Posterior compartment of the leg (deep group) |
||||
Popliteus |
Posterior surface of proximal tibia |
Lateral femoral condyle |
Unlocks knee joint; laterally rotates femur on fixed tibia |
Tibial n. (L4, L5, S1) |
Flexor hallucis longus |
Posterior surface of fibula and interosseous membrane |
Distal phalanx of great toe |
Flexes great toe |
Tibial n. (S2, S3) |
Flexor digitorum longus |
Tibia |
Distal phalanges of digits 2–5 |
Flexes digits 2–5 |
|
Tibialis posterior |
Interosseous membrane, tibia, and fibula |
Navicular, all cuneiform bones, and metatarsals 2–4 |
Inversion and plantarflexion of foot; support of medial arch of foot during walking |
Tibial n. (L4, L5) |
The following muscles are located in the anterior compartment of the leg (Figure 37-1C):
- Tibialis anterior muscle. Attaches proximally to the tibia and interosseous membrane; distally, it attaches to the medial cuneiform and the base of metatarsal 1. The tibialis anterior muscle dorsiflexes the foot at the ankle joint and inverts the foot. The deep fibular nerve (L4 and L5) innervates this muscle.
- Extensor digitorum longus muscle. Attaches proximally on the fibula and lateral tibial condyle; distally, it attaches to the dorsal digital expansions into digits 2 to 5. The extensor digitorum longus muscle extends lateral digits 2 to 4 and dorsiflexes the foot at the ankle joint. The deep fibular nerve (L5 and S1) innervates this muscle.
- Extensor hallucis longus muscle. Attaches proximally on the fibula and interosseous membrane; distally, it attaches to the distal phalanx of the great toe. The extensor hallucis longus muscle extends the great toe and dorsiflexes the foot. The deep fibular nerve (L5 and S1) innervates this muscle.
- Fibularis (peroneus) tertius muscle. Attaches proximally to the distal part of the fibula; distally, it attaches to the base of metatarsal 5. The fibularis tertius muscle dorsiflexes and everts the foot. The deep fibular nerve (L5 and S1) innervates this muscle.
Dorsum of the Foot
Muscles and their associated tendons cross the anterior surface of the ankle and insert in the foot. In addition, the following intrinsic muscles are located on the dorsal surface of the foot:
- Extensor digitorum brevis muscle. Attaches proximally to the lateral calcaneus; distally, it attaches to the dorsal surface of digits 2 to 4. The extensor digitorum brevis muscle extends digits 2 to 4. The deep fibular nerve (S1 and S2) innervates this muscle.
- Extensor hallucis brevis muscle. Attaches proximally to the lateral calcaneus; distally, it attaches to the dorsal surface of the great toe. The extensor hallucis brevis muscle extends the great toe. The deep fibular nerve (S1 and S2) innervates this muscle.
 The term “shin splints” is often an all-inclusive term used to describe pain in the anterior compartment of the leg. Most commonly, shin splints are caused by physical activity in which the foot is lowered to the ground following heel strike (such as occurs when running and especially when running downhill). The pain is due to inflammation of the periosteum of the tibia. In more severe cases, shin splints can result in stress fractures.
The term “shin splints” is often an all-inclusive term used to describe pain in the anterior compartment of the leg. Most commonly, shin splints are caused by physical activity in which the foot is lowered to the ground following heel strike (such as occurs when running and especially when running downhill). The pain is due to inflammation of the periosteum of the tibia. In more severe cases, shin splints can result in stress fractures.
Muscles of the Lateral Compartment of the Leg
The muscles of the lateral compartment of the leg produce numerous actions because some muscles cross the ankle, foot, and digits and perhaps a combination of each of these joints. The muscles in the lateral compartment of the leg have the following similar features:
- Common innervation. Superficial fibular nerve.
- Common action. Plantarflexion and eversion.
- Common vascular supply. Anterior tibial and fibular arteries.
The following muscles are located in the lateral compartment (Figure 37-2):
- Fibularis (peroneus) longus muscle. Attaches proximally to the upper surface of the fibula; distally, it attaches to the medial cuneiform bone and the base of metatarsal 1. The fibularis longus muscle plantarflexes and everts the foot. The superficial fibular nerve (L5, S1, S2) innervates this muscle.
- Fibularis (peroneus) brevis muscle. Attaches proximally to the upper surface of the fibula; distally, it attaches to the base of metatarsal 5. The fibularis brevis muscle plantarflexes and everts the foot. The superficial fibular (peroneal) nerve (L5, S1, S2) innervates this muscle.

Muscles of the lateral compartment of the leg.
Muscles of the Posterior Compartment of the Leg
The muscles of the posterior compartment of the leg produce numerous actions because some muscles cross the ankle, foot, and digits, and perhaps a combination of each of these joints. The muscles in the posterior compartment of the leg are divided into a superficial group and a deep group and have the following similar features:
- Common innervation. Tibial nerve.
- Common action. Plantarflexion.
- Common vascular supply. Posterior tibial, fibular, and popliteal arteries.
The muscles in the superficial group of the posterior compartment of the leg are as follows (Figure 37-3A and B):
- Gastrocnemius muscle. Attaches proximally to the femoral condyles; distally, it attaches to the calcaneus bone via the calcaneal tendon. The gastrocnemius muscle plantarflexes the foot and flexes the knee. The tibial nerve (S1 and S2) innervates this muscle.
- Plantaris muscle. Attaches proximally to the upper surface of the fibula; distally, it attaches to the posterior surface of the calcaneus via the calcaneal tendon. The plantaris muscle plantarflexes the foot and flexes the knee. The tibial nerve (S1 and S2) innervates this muscle.
- Soleus muscle. Attaches proximally to the posterior aspect of the tibia (soleal line) and the posterior aspect of the fibular head and shaft; distally, it attaches to the posterior surface of the calcaneus via the calcaneal tendon. The soleus muscle plantarflexes the foot. The tibial nerve (S1 and S2) innervates this muscle.


Muscles of the posterior compartment of the leg: (A) superficial dissection, (B) intermediate dissection, (C) deep dissection.
Muscles of the posterior compartment of the leg: (A) superficial dissection, (B) intermediate dissection, (C) deep dissection.
The calcaneal (Achilles) tendon is a large ropelike band of fibrous tissue in the posterior ankle that connects the calf muscles (gastrocnemius and soleus muscles) to the calcaneus bone. When the calf muscles contract, the calcaneal tendon tightens and pulls the heel, resulting in standing on tiptoe; therefore, it is important in activities such as walking and jumping. Rupture of the calcaneal tendon usually is caused by a forceful push-off during an activity such as sprinting when running or jumping in a game of basketball. The result is tearing of the tendon that connects the gastrocnemius and soleus muscles to the calcaneus bone. Bruising usually is apparent, and a visible bulge forms in the posterior region of the leg because of muscle shortening. Surgical intervention is the most common treatment.
The muscles of the deep group of the posterior compartment of the leg are as follows (Figure 37-3B and C):
- Popliteus muscle. Attaches proximally to the posterior surface of the proximal tibia; distally, it attaches to the lateral femoral condyle. The popliteus muscle unlocks the knee joint (it laterally rotates the femur on a fixed tibia). The tibial nerve (L4, L5, S1) innervates this muscle.
- Flexor hallucis longus muscle. Attaches proximally to the posterior surface of the fibula and the interosseous membrane; distally, it attaches to the distal phalanx of the great toe. The flexor hallucis longus muscle flexes the great toe. The tibial nerve (S2 and S3) innervates this muscle.
- Flexor digitorum longus muscle. Attaches proximally to the tibia; distally, it attaches to the distal phalanges of digits 2 to 5. The flexor digitorum longus muscle flexes digits 2 to 5. The tibial nerve (S2 and S3) innervates this muscle.
- Tibialis posterior muscle. Attaches proximally to the interosseous membrane and the tibia and fibula; distally, it attaches to the navicular bone, all cuneiform bones, and metatarsals 2 to 4. The tibialis posterior muscle inverts and plantarflexes the foot, providing support to the medial arch of the foot during walking. The tibial nerve (L4 and L5) innervates this muscle.
Innervation of the Leg
The sciatic nerve bifurcates into the tibial and common fibular nerves, near the popliteal fossa, to innervate muscles in the leg and foot.
The tibial nerve arises from the anterior division of the sacral plexus (L4–S3), descends through the popliteal fossa, and courses deep to the soleus muscle to innervate the superficial and deep group of muscles in the posterior compartment of the leg (Figure 37-4A). The tibial nerve descends the posterior region of the leg and enters the foot inferior to the medial malleolus to innervate the plantar surface of the foot. The tibial nerve has muscular and sensory branches.
- Muscular branches. The tibial nerve innervates the muscles in the posterior compartment of the leg (gastrocnemius, plantaris, soleus, popliteus, flexor hallucis longus, flexor digitorum longus, and tibialis posterior muscles).
- Sensory branch. Gives rise to the medial sural nerve. Branches from the tibial nerve in the popliteal fossa and descends superficial to the gastrocnemius muscle to join the sural communicating branch from the lateral sural nerve. The medial sural nerve then becomes the sural nerve. The sural nerve provides sensory innervation to the posterolateral region of the leg and foot.

A. Posterior view of the leg showing the tibial nerve and the posterior tibial artery. B. Anterior view of the leg showing the common fibular nerve and the anterior tibial artery.
Common Fibular (Peroneal) Nerve
The common fibular nerve arises from the posterior division of the sacral plexus (L4–S2) and descends in an inferolateral direction, across the popliteal fossa to the fibular head (Figure 37-4A and B). Just distal to the fibular head, the common fibular nerve bifurcates into the deep fibular and superficial fibular nerves. The following branches originate from the common fibular nerve:
- Lateral sural nerve (lateral cutaneous nerve of the leg). Originates from the common fibular nerve and courses superficially to provide cutaneous innervation to the proximal lateral region of the leg.
- Deep fibular nerve. Originates at the bifurcation of the common fibular nerve and courses into the anterior compartment of the leg. The nerve descends deep to the extensor digitorum longus and courses along the anterior interosseous membrane with the anterior tibial artery. The deep fibular nerve provides motor innervation to the muscles in the anterior compartment of the leg (tibialis anterior, extensor digitorum longus, extensor hallucis longus, and fibularis tertius muscles). The deep fibular nerve continues distally across the dorsum of the foot, and provides motor innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and provides cutaneous innervation to the skin between digits 1 and 2.
- Superficial fibular nerve. Originates at the bifurcation of the common fibular nerve. The superficial fibular nerve descends through the lateral compartment of the leg, providing motor innervation to the fibularis (peroneus) longus and brevis muscles. The nerve pierces the deep fascia to enter the anterior compartment of the leg, where it provides cutaneous innervation to the distal anterolateral leg and dorsum of the foot.
The popliteal artery is a continuation of the femoral artery. It courses through the popliteal fossa on the posterior side of the knee and bifurcates into the anterior and posterior tibial arteries at the inferior border of the popliteus muscle. The anterior and posterior tibial arteries supply blood to the leg and foot.
Anterior Tibial Artery
The anterior tibial artery originates from the popliteal artery and courses anteriorly through a proximal opening in the interosseous membrane to enter the anterior compartment of the leg (Figure 37-4B). Distally, the anterior tibial artery courses in the anterior compartment with the deep fibular nerve, crosses the anterior ankle, and continues as the dorsalis pedis artery. The anterior tibial artery supplies blood to structures in the anterior compartment of the leg as well as partial blood supply to the lateral compartment. At the level of the distal tibia, the anterior tibial artery gives rise to the following arteries:
- Anterior lateral malleolar artery. Courses laterally across the ankle joint to join the fibular artery.
- Anterior medial malleolar artery. Courses laterally across the ankle to join the posterior tibial artery.
Posterior Tibial Artery
The posterior tibial artery originates from the popliteal artery and quickly gives rise to the fibular artery (Figure 37-4A and B). The posterior tibial and fibular arteries descend deep to the soleus muscle.
- Posterior tibial artery. Curves medially, as it courses inferiorly, giving rise to the posterior lateral malleolar artery, which joins the arterial network around the ankle. The posterior tibial artery supplies blood to the posterior compartment of the leg and continues distally, under the medial malleolus, to supply blood to the foot.
- Fibular artery. Descends along the posterior region of the leg, traversing laterally to continue its descent along the medial side of the fibula. The fibular artery provides blood supply to the posterior and lateral compartments of the leg. Distally, the artery gives off a perforating branch, which courses through the inferior aspect of the interosseous membrane to join the arterial network around the ankle. In addition, the fibular artery gives rise to the posterior lateral malleolar artery, which also joins the atrial network around the ankle joint.
Anterior compartment syndrome can be caused by a tibial fracture or a high-velocity blow to the anterior compartment of the leg, resulting in increased pressure in the anterior compartment of the leg. Because the fascia covering the anterior compartment is unable to expand, pressure continues to build, causing restricted blood flow and eventual necrosis of tissues. If untreated, anterior compartment syndrome can result in amputation of the limb. Treatment varies; in more severe cases, a fasciotomy is performed and the fascia covering the anterior compartment is cut to relieve the pressure.
The veins in the leg consist of a superficial and a deep venous system.
Superficial
The superficial system consists of the great saphenous vein, located medially, and the small saphenous vein, located posterolaterally.
The great saphenous vein originates from the medial side of the dorsal venous arch in the foot and drains into the femoral vein.
The small saphenous vein originates from the lateral side of the dorsal venous arch in the foot and drains into the popliteal vein. 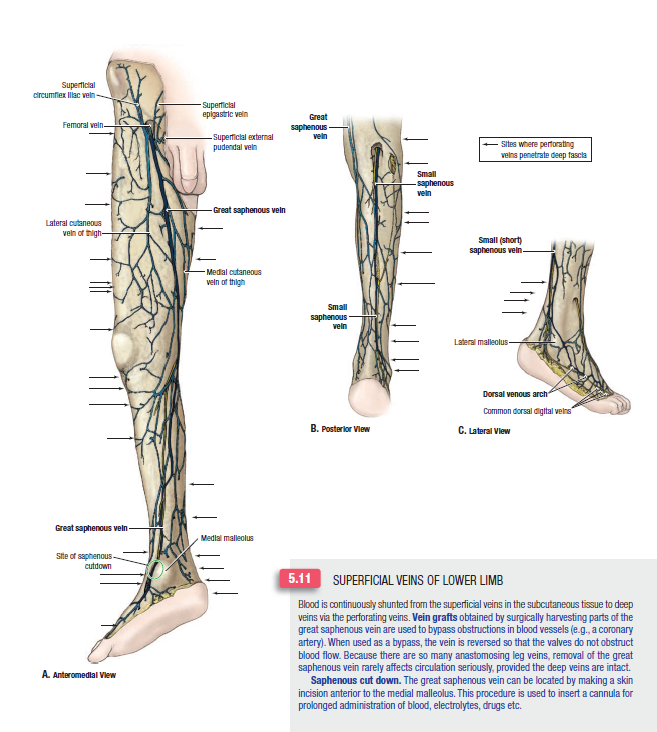
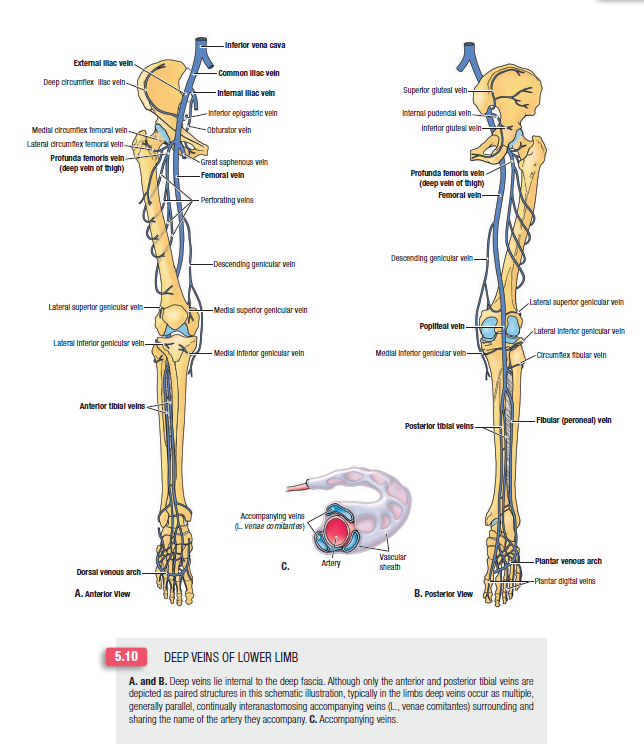
Deep
The deep venous system consists of as many as three veins, which course with each artery.
Joints of the Leg
The boney components of the leg include the tibia and the fibula, which articulate via the proximal and distal tibiofibular joints. Distally, the tibia and fibula articulate with the talus, forming the ankle (talocrural) joint. The ankle joint is a combination of articulations between the tibia and the talus (tibiotalar joint) as well as the fibula and the talus (talofibular joint).

(A) Medial and (B) lateral views of the right ankle joint.
Proximal Tibiofibular Joint
The proximal tibiofibular joint consists of articulations between the proximal tibia and the fibula. It is a synovial joint with a joint capsule, which is separate from the knee joint and is reinforced by the following structures:
- Anterior tibiofibular ligaments. Connect between the anterior tibia and the fibula.
- Posterior tibiofibular ligaments. Connect between the posterior tibia and the fibula.
- Interosseous membrane. Supports both the proximal and the distal tibiofibular joints. The interosseous membrane is strong and consists of multiple small fibers that join the tibia and fibula, proximal to distal.
The distal tibiofibular joint consists of the articulation between the distal tibia and the fibula. It is a syndesmosis joint that plays an important role in maintaining a stable mortise. The following structures reinforce the distal tibiofibular joint:
- Anterior tibiofibular ligaments
- Posterior tibiofibular ligaments
- Interosseous membrane
The ankle (talocrural) joint is a synovial hinge joint that allows plantarflexion and dorsiflexion. The ankle joint consists of articulations between the tibia and the talus (tibiotalar joint) as well as between the fibula and the talus (talofibular joint). The articulation between the tibia and the fibula (distal tibiofibular joint) forms a mortise into which the talus fits. The ligaments of the distal tibiofibular joint reinforce the mortise.
The ankle joint has a fairly weak capsule that is primarily supported by the medial and lateral collateral ligaments.
- Medial collateral ligament (deltoid ligament). A fan-shaped ligament that attaches to the medial malleolus of the tibia and the navicular, talus, and calcaneus bones. The medial collateral ligament is strong and will often avulse the medial malleolus before tearing. This ligament prevents medial distraction (eversion) and excessive range of motion.
- Lateral collateral ligament. Consists of three separate bands. The combination of ligamentous bands prevents lateral distraction (inversion) and excessive range of motion. The bands consist of the following ligaments:
- Anterior talofibular ligament. Connect between the lateral malleolus of the fibula and the posterior talus.
- Posterior talofibular ligament. Connect between the lateral malleolus of the fibula and the posterior talus.
- Calcaneofibular ligament. Connect between the lateral malleolus of the fibula and the calcaneus.
Injury to the anterior talofibular ligament due to excessive inversion with plantarflexion is the most common ankle injury. The second most common ankle injury occurs at the calcaneofibular ligament and results in anterolateral rotary instability of the ankle joint. The severity of ankle sprains is variable.